I'd much prefer we don't devolve into a political argument. My question, I thought, was relevant due to ACA kicking in, which is the first step towards universal healthcare/single payer in the US (which would eliminate the business model in question).
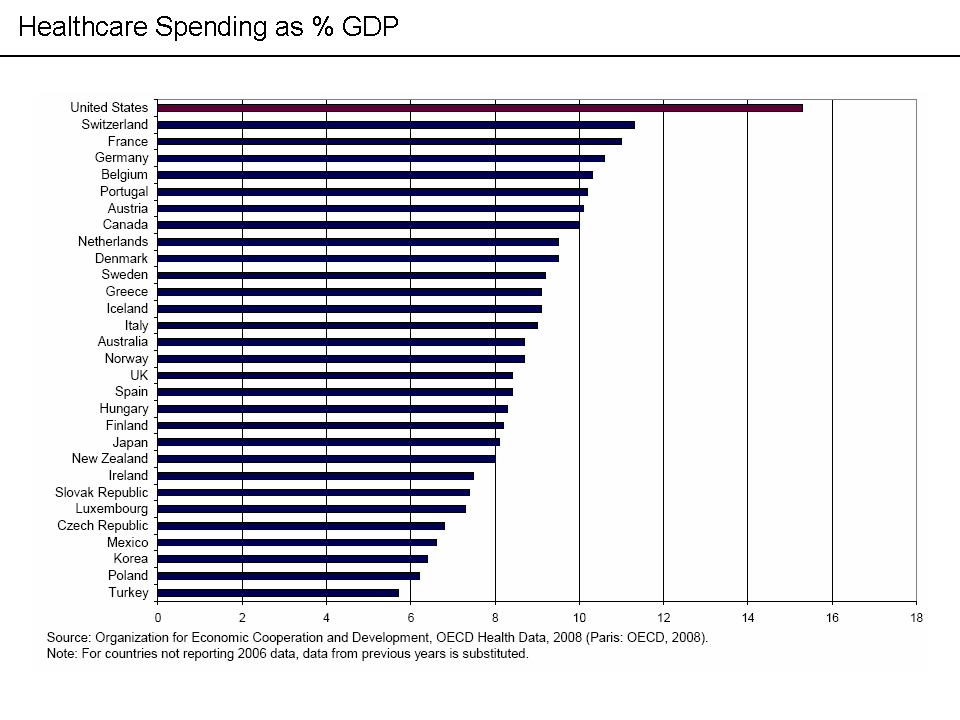
In closing, here is healthcare spending as a percentage of GDP by country (almost all first world countries): http://upload.wikimedia.org/wikipedia/commons/a/a1/Internati... The US leads in spending, and only spending.
Also, we in the US tend to have bigger problems running giant federal bureaucracies, compared to these other smaller, more-unified nations. (How many government shutdowns have they had in the past 40 years?) Our existing single-payer-ish health bureacracies, like Medicare, suffer more fraud and cost-problems, and have a harder time enforcing steely-eyed rationing (aka "death panels") than elsewhere.
These smaller systems also benefit as free-riders from positive externalities thrown off by the United States' eccentric overexpenditures - like drug and new-treatment beta-testing. (If we become more like them, their own medical indicators could get worse.)
So the argument can't just be, "make it work like over there", when nothing here works quite like there, and our challenges of scale, culture, and politics are larger.
Which doesn't explain the vastly higher per capita (and even per GDP) costs.
> Also, we in the US tend to have bigger problems running giant federal bureaucracies
That doesn't explain why the US costs (again, per capita or per GDP) are still higher than the total costs in many countries providing universal coverage even if you exclude the slightly-less-than-half of US spending that is public spending.
> Our existing single-payer-ish health bureacracies, like Medicare
Medicare isn't single-payer-ish, as for decades there has been policy to move from traditional single-payer-ish "Original Medicare" to (usually partially, with a personal premium as well) publicly subsidized private insurance "Medicare Advantage" plans.
> These smaller systems also benefit as free-riders from positive externalities thrown off by the United States' eccentric overexpenditures - like drug and new-treatment beta-testing.
Er, a lot of drugs and new treatments are tested and accepted overseas before they are in the US.
If you can't answer why Medicare seems to do worse than your favorite "single-payer-ish" models, you haven't explained how making the entire system into a single-payer system, a bureaucracy of unprecedented size, will improve things over a smaller bureaucracy that's failing at controlling costs.
Some drugs and new treatments start elsewhere. A disproportionate number start in the US. Fancy new (and often unnecessary) treatments are one of the things driving our costs up.
I see this argument all the time, and never an elaboration.
I understand going from 1,000 to 1,000,000 people incurring growing pains, but I have a hard time understanding why people seem to think a system that works for 80,000,000 people in Germany wouldn't be scalable to 300,000,000.
…isn't quite single-payer, more like a "public option".
…has far more labor-business-government cooperation than the US.
…has the oldest tradition of social insurance, but still their current system was the result of gradual expansions over many years.
…runs lots of government services better than the US.
…is only half the area of Texas, but that area is as population-dense as Maryland (our 5th densest state).
Why can't any 300 million people in Africa just adopt US-levels of public services by willpower and legal fiat? Why can't the US make our 50-million-member Medicare as efficient as the German system? These structural, historical, cultural, and political path-dependencies matter.
"Make it work because I don't understand how it couldn't" isn't a good basis for the largest nationalization experiment ever.
Those are all, arguably, consequences of the poor access to health care in this country and the short-term incentives in this country to delay care. IOW, they are products of the system that we pay more for (per capita or even per GDP -- or even either way only considering public expenditures and excluding the private costs) than first world countries that provide universal coverage through government single-payer systems.
And I really don't see the avoidance of primary care being primarily financial either. A yearly routine physical is not very expensive, and is often free at many public health clinics. Likewise common preventive care like flu shots, pap smears, and prostate exams.
A big reason a lot of people don't go to the doctor is that they don't like going to the doctor. I'm in that group. Having insurance doesn't change that.
Check out the unit cost differences here:
http://voices.washingtonpost.com/ezra-klein/2009/11/an_insur...
"But I think the biggest single driver is our fee-for-service system that rewards volume instead of value and quantity of medical services instead of quality. And as a result, we end up doing a lot of things that cause more harm than benefit for patients."
Also:
"What that dramatic variation tells us is that there's a lot unnecessary medical care that's being delivered and a lot of room to eliminate some of that wasteful spending."
Which is why almost every country outside of the US has a lower standard of care than we do. I'd be fine if we had a "minimum safety net" which covered catastrophic care, but thats not what was put into law. I also think a government mandated requirement to purchase a commercial product is probably not a good thing.
You just like to make up shit I see. Every country that provides public healthcare has a higher standard of care than we do because for 10's of millions of American's there is no care at all beyond emergency care. People die daily for lack of health care in this country, to call that a higher standard than countries with public healthcare is beyond absurd. Our system has a fantastic standard of care for those with money, it has shit for care for the rest.
Uh, where do you get that from? The JAMA study, one of the most comprehensive such studies done, concluded that the US health care outcomes are far worse than comparable nations, yet we pay significantly more for it.
The biggest reason we pay more is that provider costs are much higher than the GDP-adjusted average. $500,000,000,000 more. (And before you say it, that's factoring out defensive medicine and the results of tort reform.) A lot of that has to do with insurance companies inability to negotiate reasonable rates with the providers. And of all the insurers in the US, which is the only one that can and does negotiate reasonable rates? Medicare.
Every first world country except the US has something approximating universal coverage, but not all of them use single-payer (or even a single basic coverage insurer with supplemental coverage from other payers.) Compulsory-purchase insurance models similar to those in the ACA (but, you know, actually universal) with private insurers are not unheard of (e.g., Switzerland uses that model)
{kind=link}