> With California leading the way, a handful of states are considering trying to disrupt the market for essential medications, starting with insulin. The plan would be to manufacture and sell insulin themselves for a price that is roughly equivalent to the cost of production.
I feel like I'm missing something here. My understanding of why insulin is so expensive: laws are created and enforced by the government preventing people from competing in the space.
If you try to make your own insulin, and you take it to market with 3rd party analysis and certification of it being medical grade (and safe) insulin, you'll start seeing an escalation of the state against you. First angry letters from lawyers and eventually, if you continue head strong and ignore everyone telling you to stop, government officials (possibly with guns) will come and forcibly shut you down.
Is California just going to ignore these laws? How will the state not be liable for damages when individuals are?
I'm all in favor of revoking the legal structures that pick the winners in this market. It seems like there are plenty of people passionate in this space that would/could make insulin at near-cost if permitted to.
It's just that, by my understanding, it's the government that doesn't permit them to. It's weird that people in the government (at the state level) are stepping in to do what people in the government (at the federal, but possibly also the state level?) won't let people in the market do.
Edit: substituting “intellectual property laws” with “laws” as it seems there’s more to it than just IP.
California, on the other hand, is paying a lot of money to Novo Nordisk et al, and would benefit from reaching a low average price. They can afford to go through the approval process with all the important insulin analogs. And they won't go bankrupt in court before it pays off.
In the U.S.A. is expected to expire on 2027-07-05.
How did something invented in 1994/2000, get patented in 2009? https://patents.google.com/patent/US8048854B2/en%3C/
That is incorrect. A bioequivalence study is much simpler and cheaper than the original safety and efficacy studies.
You do not need to prove that safety and efficacy of the drug, only that you are delivering the equivalent of the originally studied drug at the same doses.
That’s not an accurate understanding of intellectual property specifically. Insulin isn’t like a pill, where once you have a chemical formula you can make millions of them very cheaply. It’s a biologic, an artificial hormone. Even leaving aside the patents, it’s very expensive to get approval for a generic biologic (called a biosimilar). That’s why there are few manufacturers of synthetic human insulin, even though that’s out of patent.
Another obstacle, as you pointed out, is that there are few manufacturers who produce synthetic insulins. From what I've learned in my discussions with manufacturers is that many are transitioning their facilities to a focus on mRNA drug manufacturing. Therefore there is a limited set of manufacturers who don't make insulin but have the equipment/facilities for it (in the U.S.).
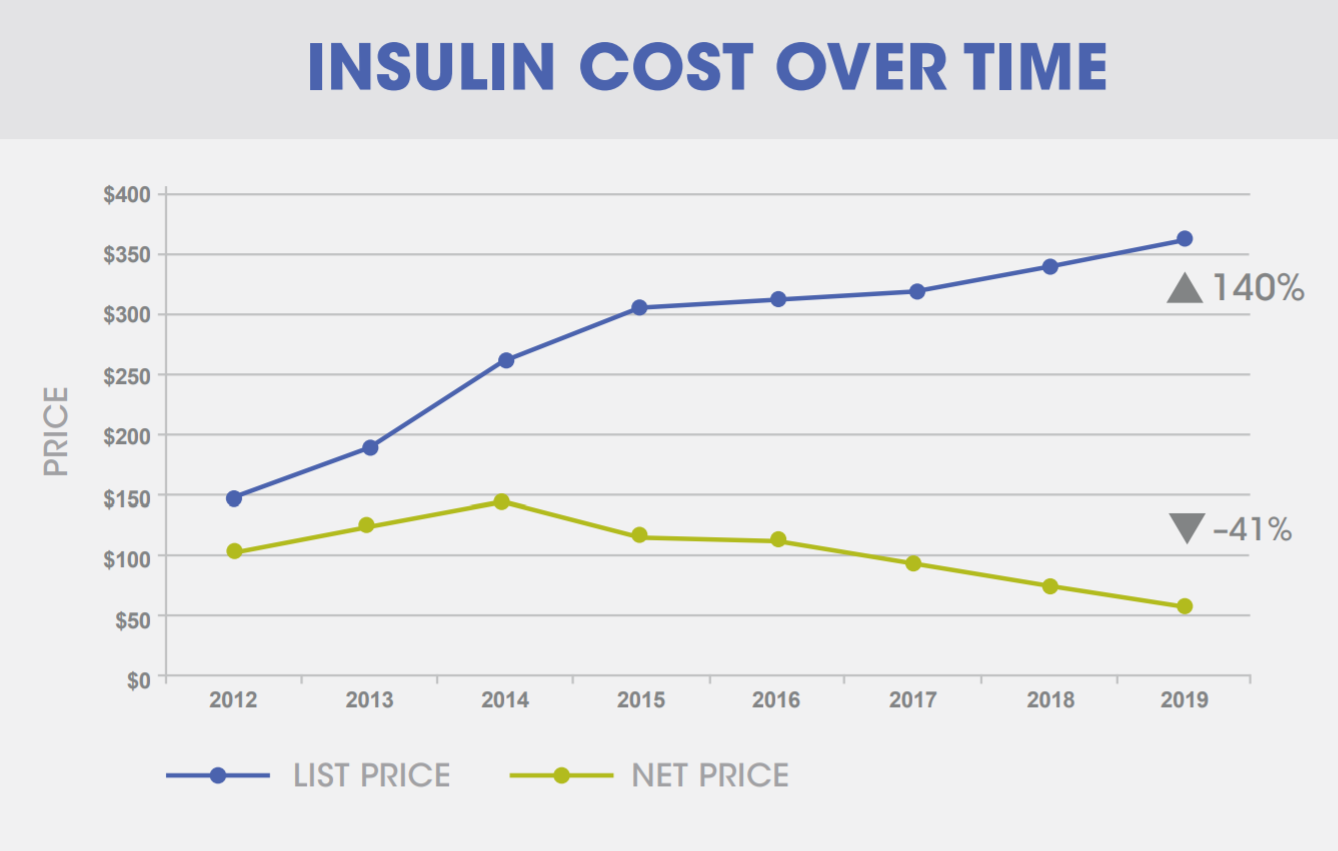
>Average retail prices of Novolin and Humulin (traditional short- and intermediate-acting insulins) have gone down, or held steady, while prices of modern rapid- and long-acting insulins continue to go up. On average, traditional insulins now cost less than half of what modern insulins cost.
https://www.goodrx.com/healthcare-access/research/how-much-d...
There is a lot more going on that makes high end insulin expensive. A lot of conversation around insulin is people talking past each other because they are referring to different things that they think should be free, usually one of these additional features on top of the hormone itself.
I suspect they would be breaking federal laws, so I believe consideration of the State's 10th Amendment rights applies here. That would be wonderful and hope that this case brings that topic into the spotlight, because I see 90% of the federal government as being grossly unconstitutional on that basis alone.
Personally, I suspect the market leaders would not want to face the courts, because the exposure would be horrible PR that affects all of their product lines. Moreover, an aggressive and concerted effort to block this effort should be viewed as the anti-competitive behavior of a cartel, which is the status quo de facto that the State is effectively trying to disrupt.
I don't see such a challenge as anything but a lose-lose for those companies. Hopefully, they take the bait and do something stupid that leads to reform at the national level.
An interesting wrinkle is that Congress already foresaw this and passed a law decades ago waiving state sovereign immunity for patent and copyright claims. But then SCOTUS overturned the patent prong of this federal waiver on the grounds that Congress hadn't proven that states had a pattern of telling patent holders to go fuck themselves. And SCOTUS's reasoning for striking down the suit about Blackbeard's Law was that this also held true for the copyright prong of that law... despite being handed a brazen example of a state nullifying copyright law for their own gain on a silver platter.
What this technically means is that your state could, tomorrow, run their own pirate streaming site and not get sued for it[1]. The only way to stop it legally would be to sue end users, which would be difficult to do for a direct download service[2].
As for antitrust and cartels, since copyright and patents are legal, government-granted monopolies, most courts are very loathe to attack them even when they are used in ways that violate antitrust law. You can see this in FTC v. Qualcomm, where an appeals court smacked down an antitrust ruling for this reason. Compounding this is the fact that a very large contingent of judges have been slowly nullifying antitrust since the 1980s under the "consumer welfare" theory that every tech company is built to maximally exploit.
I could see California getting away with bloodying Eli Lily & Co's nose. But I would not count on this becoming a future model for evading (ab)use of the patent system. Remember, all the states are still part of a federal government that is very much in favor of the patent system as currently constituted, and there are still things they can do to block California.
[0] https://nsglc.olemiss.edu/blog/2020/apr/2/index.html
[1] Assuming your state had not already waived sovereign immunity for copyright
[2] It's commonly believed that you can't sue for downloads, only uploads. This isn't quite true. At least one court has outright said that both are illegal but infringe on different exclusive rights. I don't remember which court.
Insulin can be made without breaking patents. Unless you specifically require something branded as Lantus®, for example(which is in no small part due to publications funded by pharmaceutical companies themselves, but also some 'marketing' straight to doctors). There are other longer lasting insulin formulations that can be made.
There are hurdles if you take that route (as described in the article). Many are financial. One is regulatory (biosimilars).
> Other federal regulations have added to the challenge. The FDA began to treat insulin as a biologic drug in 2020 — meaning it is made with living materials instead of combining chemicals like conventional pharmaceuticals — which comes with a different set of standards for generic versions, which are known as biosimilars, as well as manufacturing challenges given the precise conditions these products must be made in. Biosimilars can cost up to $250 million to produce and take up to eight years to bring to the market, versus a one-year investment of as little as $1 million for conventional generics. And unless the FDA recognizes a new generic insulin as interchangeable with the products already on the market, health insurers might not want to cover it and doctors may not be willing to prescribe it.
Seems like the barriers for a state entity are exactly the same as the barriers for private generic drug manufacturers, and the state could easily just stop erecting these barriers.
The ability to mass produce insulin at negligible cost has been around for decades, they guy who discovered it made it patent free even.
Only in the US do companies get away with this kind of price gouging, and only because of monopolistic (or I get oligopolistic?) behavior and BS legal threats against anyone that might impact their profiteering off the work of others (paying off competitors not to compete, and BS patents on minor changes, with applications carefully scattered to maximize length of coverage).
The only reason it's taking someone the size of CA to actually do something, is because the Pharma companies buy out, pay off, or lawyer into oblivion anyone else. All strategies that normally work because the victims of the (to me) clearly illegal monopoly based actions aren't incurring costs if they stop, whereas the gouging and monopoly tactics cost CA huge amounts annually. The only thing Pharma could do to make it worth CA not doing this would be to stop price gouging, which is of course the only reason CA is doing this.
That price gouging is illegal if it's some dude hoarding toilet paper, but not when it's insulin being sold by multi-billion dollar corporations remains absurd. That people come to defend the "IP rights" of these organizations and their BS patents is a really American phenomenon.
Long acting insulin is not.
They are different products, and the formers patent being free has nothing to do with the later innovations being locked down.
There is no patent on insulin, just regulatory capture on which proprietary analogs are approved for medical use. In 2020 the FDA changed the regulatory status of insulin, signaling that it's not going to let that regulatory capture continue. But if it does, there will be a lawsuit, it will go to the Supreme Court, and the pharma companies' arguments will probably get thrown out.
The issue is that while insulin is actually quite cheap to make once you get started, the startup-costs associated with getting to that point are quite hefty: lab real estate, equipment to make and purify, FDA fees, etc.
Newer versions of insulin are "better" than generic insulin: easier to take, fewer side effects, etc. The major insulin producers have been slowly doling out minor improvements over time, about every decade or so, to maintain IP protection on these newer modern versions of insulin, and the high prices associated with these newer versions. They've also been paying off several generics manufacturers to delay them from manufacturing generic versions of these modern versions as the patents expire.
Even that is debatable. At least Sanofi has been known to fund some rosy articles about their Lantus® product. When the EU looked into it (for similar initiatives) they were not able to find the large 'performance' gap that was suggested between that insulin and alternatives.
Isn't that already illegal (price fixing/collusion)? How are they structuring the deals to avoid prosecution?
This is 100 year old technology. It has nothing to do with development cost.
https://www.vox.com/2019/4/3/18293950/why-is-insulin-so-expe...
The article doesn't do a good job of explaining that "insulin" isn't a single drug, or at least how they describe it.
Generic insulin is cheap. You can get it for $25/vial from your local Walmart. With production costs, regulation compliance, storage, transport, and paying pharmacists, they're not making much profit on that.
Patented insulin analogs are not cheap. They have different characteristics for duration and onset time that make them easier to dose, but the patent means that you can't produce and sell it unless you own the patent or have licensed it. Drug companies who own these patents set their prices according to what they can get insurers to pay, not according to what they expect people to pay out of pocket.
One of the weird quirks of the US medical system is that drug companies often have alternate prices for people without insurance. Remember, the high prices aren't designed for you to pay, the high prices are designed to extract as much money as possible from your insurance company.
You can see this in action on drug company websites. Lilly has a program that will cap your payments at $35 for even their expensive insulin analogs: https://www.insulinaffordability.com/ You have to renew every 12 months and hope they're still doing it, but they generally keep these programs around because it dampens the outrage about the high prices.
California will make insulins already off patent. Ones where lower cost versions are already available. It would be far smarter to just subsidize existing versions.
But it doesnt solve the problem that the latest cutting edge patented insulins cant be copied by the government.
1. Centralise power in a regulatory body that will raise costs every time something goes wrong.
2. The barrier to getting things done rises until there is a crisis.
3. The barrier is so high only someone behaving like a financial illiterate would enter the market, so legislators task government with entering the market or underwriting someone who can.
So I'd assume that legal ability that was ever the problem. Usually it is regulatory requirements implying a minimum size of the actor needed to take on the risk. I see a few comments that this time around the technical term implementing this for insulin is "bioequivalence" but the broader pattern applies in a few markets and should be called out.
IANAL. But would this be similar to Jim Olive Photography v. University of Houston System?
https://fairuse.stanford.edu/case/jim-olive-photography-v-un...
Like they ignored asinine federal drugs laws? I hope so!
Rather, the executive branch of the federal government is choosing to not enforce federal drug laws (in some situations, for some drugs).
Federal agents can walk in and charge everyone in a cannabis store anytime they want, as I understand it.
Municipal broadband, power, roads, schools, post, housing, and healthcare? It's long overdue, and with an appropriate amount of funding has been shown to be effective at controlling costs and delivering moderately good quality in most cases.
A lot of things get so warped by profit motive. And there are places I want a profit motive, but insulin (and healthcare generally) isn't one.
Yeah, everything was great under the state owned telco monopolies. Let's get back to that!
Where? The US has among the highest percentage of kids going to government owned and operated schools. We have plenty of government housing as well (projects). Nearly all of our roads and transit systems are publicly owned and operated too.
Almost uniformly, those government operated systems aren’t very good—in America. And it doesn’t have to do with “funding.” If you compare with Europe, we spend more money per student, per transit rider, and per public housing resident, etc.
Municipal broadband: the best broadband in the entire United States is provided by the municipality of Chattanooga. [1]
Post: The USPS is the most trusted brand in the United States, above FedEx and UPS. [2]
Transit: The New York City Subway is the 3rd largest metro rail system on earth after London and Guangzhou. Ok fine, it's expensive to build - but it moved 1,300,000,000 people in 2021.
That's just three random ones.
[1] https://www.ama.org/marketing-news/usps-ranked-most-trusted-...
[2] https://qz.com/1996234/the-best-broadband-in-the-us-is-in-ch...
The profit motive coupled with competition works very well to keep prices low.
You need only realize the following; European firms stand at the ready to supply insulin at well below US prices today, but are prevented from doing so by the FDA. And they can do so and still turn a profit.
That has never happened. What does happen is the cost is borne by the taxpayer rather than the user of the service.
The "warping" of the profit motive in the insulin case is entirely caused by government interference and regulation (by making it nearly impossible for competitors to spin up and make insulin).
If the state takes a commodity and sells it on a cost plus or cost basis, it’s going to kill investment in the spaces and collapse the margin.
At this point, we’re killing people and bankrupting states and employees with out of control costs. Making an example out of insulin would fix that and constrain some of the players in the market.
If the service is "not dying preventably" that's fine.
https://theconversation.com/why-telling-people-with-diabetes...
Walmart also sells, and has for a while, "regular" human insulin under their "ReliOn" brand, which is $25/vial. This is an older style of insulin, less flexible and reactive, and requires a more restrictive lifestyle to make it work . Not following this restrictive diet schedule and rules can put you at risk of a hypoglycemic incident, which can be fatal.
There are other kinds of insulin analogs, including a "slow acting" variety called insulin glargine (sold under the brand names Basaglar, Lantus, etc). It serves to smooth the overall curve of blood sugar on a given day. My own treatment regime includes both insulin aspart and insulin glargine. I do not believe Walmart sells any insulin glargine (yet?)
For what it's worth, as an additional piece of information, a Continuous Glucose Monitor (CGM) is another modern tool in the treatment arsenal. They are also incredibly expensive, especially without insurance, but have saved my life several times when I made mistakes or just had bad luck with a dose of insulin aspart, and went very low. Being able to see myself starting to go low, rather than simply reacting when it is too late and I am already affected, is a significant aid.
Hopefully California is planning on doing a different style of insulin that better manages that?
https://theconversation.com/why-telling-people-with-diabetes...
There's no reason California couldn't say, "If you need insulin, and you live in California, it's available for free." Assuming that's what the taxpayers want.
Governments are just collections of people organized by incentives, just like corporations.
In corporations, the profit incentive pushes the organization to minimize the cost of production. At the same time, competition puts a ceiling in prices. Poorly organized, staffed and managed businesses go bankrupt.
In a government, there is no incentive to minimize costs. Next years budget is contingent on isi h all of this years. Leadership positions are politically appointed, not based on competency. Employees are not rewarded with huge bonuses or promotions for competing projects on time or ahead of schedule. Budgets can just be sink holes, as long as they are politically expedient and have the proper messaging. Better ideas are routinely stifled by political agendas, and investment is singular; one department gets all the funding and there is no competition.
Look at Venezuela as an example. When the government nationalized the oil industry, it completely fell apart. Production dropped off hugely.
My understanding is that it is manufactured by Novo Nordisk, the makers of more modern, name-brand insulins, as well (they make the fast-acting insulin aspart called Novolog that I take as part of my own regimen).
For further reference: https://diabetesstrong.com/walmart-insulin/
That's what my brother used to take 20 years ago.
They are not exactly 'inferior technology' and there are uses for them. But you are right that diabetics these days don't generally take them.
There are generic long lasting insulin alternatives, but none that I know of are available in the US. I believe that's what CA wants to do.
Walmart sells human insulin (the previous gen stuff) for $25/vial. It’s manufactured by Novo Nordisk. It’s what was regularly prescribed in the 1990s. It has downsides, such as requiring a strict eating schedule: https://diabetesstrong.com/walmart-insulin/
Most doctors today prescribe human analog insulin. They do this because it is better at controlling blood sugar without requiring strict eating schedules.
whatever the quality of life improvements of the newer stuff is its worth pointing out there's a doctors-getting-kickbacks scandal every few years https://duckduckgo.com/?t=ffab&q=prescription+kickbacks&ia=w...
It looks like one party tried to get this done in reconciliation. If so, blaming “arcane rules” is slanted and makes me wonder what other information the author is twisting.
I would say that whole combination is pretty arcane.
Sure, at a high level it's simple. But so is "crawl the internet, make a database and match keywords from requests to a ranked list of results."
Sorta. They can be fired at will (https://www.washingtonpost.com/archive/politics/2001/05/08/k...) and they're making advisories, which the Senate can just... overrule.
https://www.axios.com/2022/08/07/insulin-price-cap-reconcili...
There was little reason to block it and it is hard to imagine why they blocked it given how many people it could help. I tried to understand the logic but most everything I read were just out right lies. I have knowledge of this first hand because my wife takes insulin.
I do agree that it's on-topic in this particular thread to have a discussion about the merits of policies like this and that can include highlighting the factions that support or oppose them (and the reasons and/or incentives that might be driving that support/opposition).
One should look at their own employers and see if everything they are doing is ethical.
NOTE: just making a point, I don’t condone what these companies are doing
Type 1 diabetes has nothing to do with diet it is an autoimmune disease with genetic and possible environmental antecedents.
If you're interested in learning more about type 1 diabetes please check out:
https://mises.org/wire/patents-legal-monopolies-and-high-pri...
The FDA, from my perspective, plays such a huge and important role in our society and showcases the exact things we need from our government. They are an example of a government entity that mostly gets the job done right, an essential part of our livelihood today.
In 1960, Richardson-Merrell applied for approval for a drug called Thalidomide, a cancer treatment. They had clinical trials that included pregnant women. They were rejected six times.
In the UK, The Distillers Company (Biochemicals) Ltd, a subsidiary of Distillers Co. Ltd marketed thalidomide as Distaval, a remedy for morning sickness. Their advertisement claimed that "Distaval can be given with complete safety to pregnant women and nursing mothers without adverse effect on mother or child ... Outstandingly safe Distaval has been prescribed for nearly three years in this country."
By 1962, over 10,000 children (most in west germany) were born with crippling disabilities caused by thalidomide. Over 2,000 died.
Frances Oldham Kelsey was awarded the medal for Distinguished Federal Civilian Service by President John F. Kennedy for rejecting the drug.
It also tries to blur between patents and exclusivity. Exclusivity is usually 3 years (5 for new antibiotics and new chemical entities). Patents are 20. Exclusivity is a very small portion of intellectual property protection. I would call that dishonest.
The FDA does not control drug patents, the patent office does. Abolishing the FDA would do practically nothing to reduce IP protections, but would eliminate all the other things they do, like making sure drugs work and don't kill people.
Like they did with Thalidomide?
Abolish both the FDA, and IP.
About 3 in 4 enrollees in ACA plans that use insulin pay $35/month or less out of pocket. For people with private insurance, 4 in 5 pay $35/month or less.
The biggest problem seems to be too many plans, too many choices, and too many ways to fall through the cracks.
It's still a despicable racket if the patient only pays $35, but the insurance company is paying $500.
Folks in the Type 1 boat are in a much rougher place without insurance than the far larger, and growing, population of Type 2s. And I imagine, skew any reporting that does not make the discrimination between the two.
(This all intended as a supplement to your very good point)
As if the federal government isn't the one causing the shortage in the first place.
# 1 competition works
> When a company develops a new drug, it gets a period of exclusivity, 10 years or more, in which it is the only one able to make or sell that drug. But after that exclusivity period has passed, other companies can make a carbon copy and sell it at a lower price. Studies find that once several generic competitors come on the market, prices drop significantly.
# 2 big pharma has hacked regulations for prescription drugs, medical devices and generic replacement to prevent losing federal government granted monopolies.
> But pharma companies are savvy about finding ways to extend their monopolies, with insulin and other drugs, by making minor tweaks to the chemical compound and asking for a patent extension. In the case of insulin, the companies can also modify the delivery device to protect their market share. Each product is meant to be used with specific, company-designed injectors.
This is a government created problem.
https://worldpopulationreview.com/country-rankings/cost-of-i...
https://1.bp.blogspot.com/-ZfBANMMU5dQ/XzFtNw93ZCI/AAAAAAAAq...
Insulin is cheap. My brother gets his from the Brazilian government, no charge and no proof of income(it is a life-saving medication and you already pay your taxes). If you want more "convenience" (receive at home, not wait in line, etc), you can go to a pharmacy and pay. Costs maybe $20 for a month's supply of brand name long acting insulin (less if you are low income, even less if you have some forms of private insurance).
The Brazilian government also highly incentivizes generics vs brand names, doctors will often prescribe by the active ingredient unless there's a very specific reason to go to a particular brand. It has threatened to break patents (and done so on occasion) of companies that overcharge for essential medication (https://www.reuters.com/article/us-merck-brazil/brazil-bypas...)
There is absolutely no way insulin costs should be as high as they are. Walmart survives with a 3% profit margin but somehow we allow pharmaceutical companies to charge about whatever they want. It's not 'high tech' anymore, despite minor improvements by Lilly and friends to keep the patents alive.
Related: US health care costs (global is following) are also higher than they should because of the food industry. They will push their sugar heavy processed crap worldwide, but in the US they use high fructose corn syrup. For decades fructose was erroneously pushed to diabetics because fructose doesn't raise insulin levels. What it does do it cause metabolic syndrome, ultimately leading to obesity, type-2 diabetes, and there are links to cancer and even a growing number of publication linking to Alzheimer's and dementia in general. 88% of Americans have some sort of metabolic dysfunction(https://www.ksl.com/article/50332891/88-of-americans-are-met...).
We tend to shame people and say that they are pre-diabetic, obese or what have you because they are lazy and over eat. That's untrue. You can't outrun a bad diet. People will try to "eat healthy" and eat a bowl of cereal because companies say it's good for you. It is not. They will cut fat (and end up eating more carbs) because they have been told (by the food industry) that fat is bad. It is not, sugar and highly processed foods are. They feed people bad information(a calorie is a calorie) and then shame people for not "taking care of themselves", all the while polluting geniune research that contradicts them. It's terrible.
The same free market entities that produced covid vaccines in record time?
That free market?
"Domestic manufacturing" is just a talking point to fig-leaf the real goal.
Hang on, isn’t insulin pricing the exact sort of thing anti-cartel/anti-competitive laws are meant to prevent?
I thought thr Indian pharmaceutical industry was well able to make it, why not just buy it?
Seems like a very roundabout way when we could just ignore intellectual property laws directly, at home. The same applies to "importing things from Canada." Why the ruse?
It is out of patent.
[...]
> But in the long term, the plan is for a government factory operated by government workers producing government-owned medication. The state would have its own public production facilities, staffed by civil workers, which would sell generic insulin for the same cost needed to produce it, plus perhaps a small percentage to cover auxiliary costs for the program.
> The $100 million in funding is split evenly between the short and long term. But that long-term vision will take time. Even if the state were to retrofit an existing factory for insulin production, that construction work could take years, as would hiring a workforce to oversee it. Once production is up and running, California would need to hit more targets — most importantly producing a product that the FDA says is interchangeable with existing insulin medications.
That second phase is certainly ambitious. Putting it out for bid would be the more normal government process. It will be interesting to see what happens.
https://news.ycombinator.com/item?id=32021868 (216 comments)
I clicked on the Vox link, hoping to see an update. There wasn't one, although I'm guessing that the 2022 announcement was about the budget being approved and now in 2023, they just started writing an RFP.
TL;DR: "Evergreening is any of various legal, business, and technological strategies by which producers (often pharmaceutical companies) extend the lifetime of their patents that are about to expire in order to retain revenues from them. Often the practice includes taking out new patents (for example over associated delivery systems or new pharmaceutical mixtures), or by buying out or frustrating competitors, for longer periods of time than would normally be permissible under the law."
A relevant quote from the Wikipedia article: "In one study of the prescription drug market, Feldman found that 78% of new patents associated with prescription drugs were for existing drugs."
Depressing AF...
1. https://www.t1international.com/blog/2019/01/20/why-insulin-...
What a reality. I‘m glad that I don’t have a life threatening diseases, but I would do everything that is possible to survive. Steal, rob, fraud to come at least up with the money to survive.
I‘m shocked that simply surviving a manageable sickness in a first world country is not a human right.
1. https://slatestarcodex.com/2016/08/29/reverse-voxsplaining-d...
2. https://slatestarcodex.com/2015/09/24/the-problems-with-gene...
I hope this is done well.
Her HbA1c long-term blood sugar measurement was literally off the charts. Off the chart on the wall on the hospital, right through the red “DANGER” section. She had lost 17% of her bodyweight and half of her hair.
We have learned the following:
You want a continuous glucose monitor (CGM), and an insulin pump, with rapid-acting insulin.
You do not want long-acting insulin. Especially not insulin glargine. It is a dangerous form of insulin: It is injected as a blob of insulin (“bolus”) under the skin. It’s supposed to stay in the place and slowly fritter and diffuse into the bloodstream. This effect is due to crystallization of the modified insulin amino acid chain in the pH level inside the body. It’s clever. However, if insulin glargine happens to go into a blood vessel, it works pretty much instantly. Then it is not long-acting at all. The subcutaneous environment is… living tissue. There are capillaries. It can and will go into directly into the bloodstream at some point. For some reason. At injection time, or due to bumps and jostles and physical pressure. Then there are no brakes on it. 24 hours’ worth of active insulin can go into the bloodstream. Then every cell in the body is signaled hard to pull glucose from the blood – all the flesh in the body rips the sugar out of your blood, leaving too little for the brain. People start losing consciousness in minutes, csn pass out, and may die.
Insulin degludec is another long-acting insulin, one which is acceptable in this regard. The bolus stays glommed together due to polymerization of the insulin so it’s more robust. It also has molecular brakes on it kind of – if it does go into the bloodstream, it attaches to albumin in blood plasma and doesn’t become active all at once.
However, using rapid-acting insulin in a pump is strictly better because this replicates the insulin oscillation of the pancreas. “[The pancreas’] basal insulin level is not stable. It oscillates with a regular period of 3-6 min. After a meal the amplitude of these oscillations increases but the periodicity remains constant. The oscillations are believed to be important for insulin sensitivity by preventing downregulation of insulin receptors in target cells. Such downregulation underlies insulin resistance, which is common in type 2 diabetes.”—https://en.wikipedia.org/wiki/Insulin_oscillation
The insulin pumps work this way. They pump the insulin with a rhythm. It’s easier to control the blood sugar and you need less insulin. It’s crucially different and much better for long-term health and quality of life.
The most important things are a good blood sugar sensor (continuous glucose meter or CGM), and a good pump with a good user interface. We haven’t tried one of the closed-loop automatically controlled pumps that reads from the sensor and autoadjusts, but it’s clear from the problems people have with badly designed pump that a good “semiautomatic” pump is better than a poor and unpredictable sensor-feedback-controlled automatic one. These have issues like sometimes cutting out without giving clear warning if blood sugar is high, and the blood sugar target range can’t be adjusted low enough (liability issues afaik) so people tend to stay at too high blood sugar levels which do long-term harm. I do assume that a good automatic pump is magic.
Also, glucose metabolism and inflammation are intimately related, which ties into the vascular system. There is a lot more actionable science out on this than most doctors are aware of. (Overburdened medical personnel are unable to keep abreast of scientific developments.)
{kind=link}